

Non-Celiac Gluten/Wheat Sensitivity
If you react badly to gluten but your celiac blood tests came back negative. Or if you’ve never been tested, you’ve probably been told, in one way or another, that what you’re experiencing isn’t real. Maybe by a doctor. Maybe by an article online. Maybe by a relative who finds your eating habits inconvenient at family dinners. Non-celiac gluten sensitivity is real.
Non-celiac gluten sensitivity (NCGS), also called non-celiac wheat sensitivity, is a recognized clinical entity. Researchers, including Alessio Fasano (Harvard/MGH), Umberto Volta (Bologna), Carlo Catassi, and Detlef Schuppan (Mainz), have spent more than a decade documenting it.
The Salerno Experts’ Criteria, published in 2015 by an international consensus group, set out a structured approach to clinically identifying NCGS. It exists. The science is messier than celiac science; the diagnostic criteria are still evolving, and the prevalence estimates vary widely. But the condition itself is no longer seriously in doubt.
This article walks you through what’s known, what’s contested, why diagnosis is so difficult, and what to do if you can’t get one. Or have chosen not to seek one. It’s the article I wish I’d had during my own decade of going gluten-free without a formal diagnosis.

A Note on My Own Gluten Sensitivity Story:
I’ve never had a formal celiac diagnosis, but I’ve lived strictly gluten-free for years after an elimination diet lifted symptoms I’d carried since childhood: short stature, migraines, joint pain, exhaustion that never quite matched my life. I treat myself as celiac, with no “just a little” and no risk-taking with cross-contamination.
(You can read the full story of why I never got tested, and the diagnostic gaps that leave 70–80% of celiacs uncounted if you want the longer version in Newly Diagnosed Celiac – Now What? ) Whether you’ve been formally diagnosed, told you have non-celiac gluten sensitivity, navigated a false-negative result, or are quietly certain your body reacts even when the paperwork doesn’t match, this space is for you.
What Non-Celiac Gluten Sensitivity Actually Is?
NCGS is defined by what it isn’t, which is part of why it’s so contested. The current working definition: a clinical condition in which symptoms are triggered by ingestion of gluten-containing foods, in the absence of celiac disease and wheat allergy.
That means negative celiac antibodies (tTG-IgA, EMA, DGP), normal duodenal biopsy on a gluten-containing diet, negative IgE wheat allergy testing, and yet, when gluten is removed, symptoms resolve and, when reintroduced, they return.
Common symptoms include:
- Bloating, abdominal pain, altered bowel habits
- Brain fog, fatigue, headaches
- Joint and muscle pain
- Skin issues: eczema, dermatitis, unexplained rashes
- Mood symptoms: anxiety, low mood, irritability
- Numbness or tingling
If that list looks broad and overlapping with celiac, that’s because it is. Symptomatically, NCGS and celiac can be near-identical. The difference lies in the underlying mechanism, the long-term complications, and the diagnostic markers.
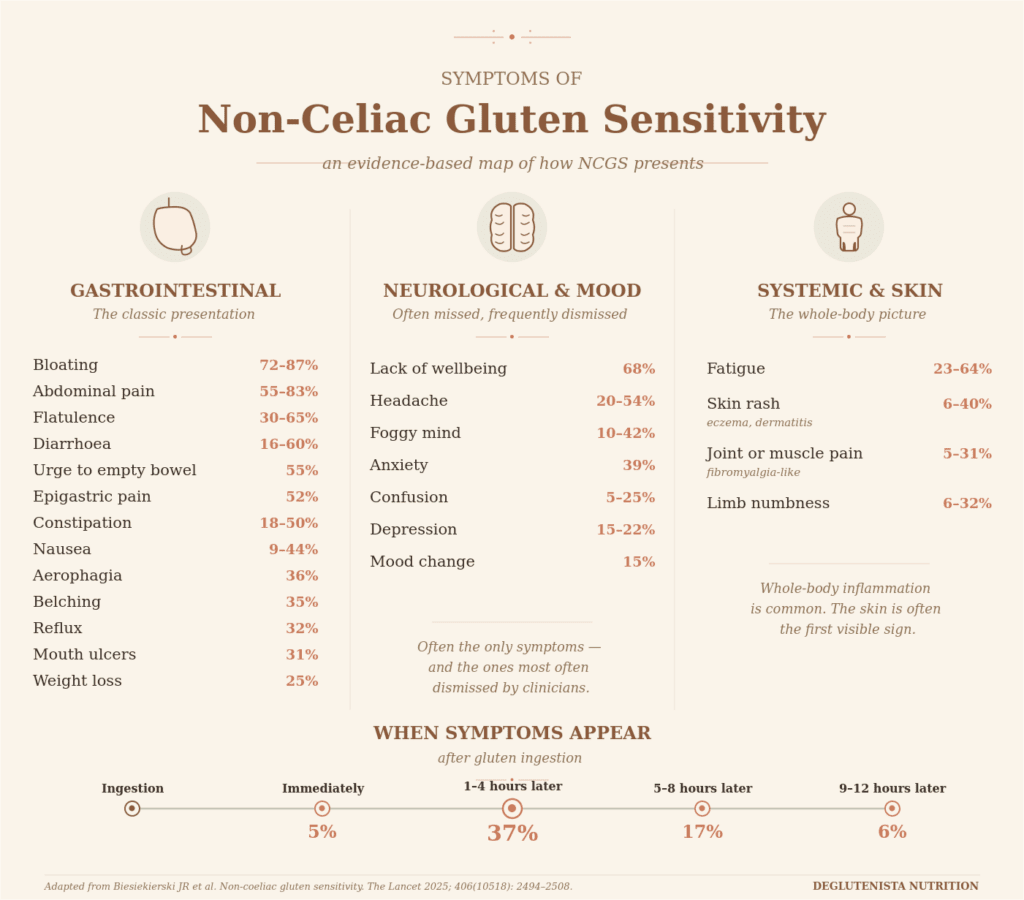
Non-coeliac gluten sensitivity The Lancet 2025
Why is Non-Celiac Gluten Sensitivity Diagnosis So Hard?
Three reasons NCGS is genuinely difficult to diagnose:
1. There’s no biomarker
Celiac has antibodies, genetic markers, and a visible duodenal lesion on biopsy. NCGS has none of these reliably. Researchers are working on candidate biomarkers, auch as fatty acid binding protein (FABP2), lipopolysaccharide-binding protein, and anti-gliadin antibodies of the AGA-IgG type. However, nothing has reached routine clinical use yet. Diagnosis is currently made by exclusion of celiac and wheat allergy, plus a structured gluten challenge.
2. The gluten challenge is brutal
The gold-standard diagnostic process is the double-blind placebo-controlled gluten challenge requires reintroducing gluten in capsule form for one to two weeks, then a placebo, then comparing symptom diaries. For someone whose body has spent years recovering from gluten, voluntarily triggering symptoms again is a serious ask. The Salerno criteria recognize this; even formal research protocols struggle with patient adherence. In real-world clinical practice, very few people complete the full challenge.
3. The label keeps shifting
Some researchers prefer “non-celiac wheat sensitivity” because it’s not always clear that gluten itself is the trigger. Wheat contains other potentially reactive components: fructans (a FODMAP), amylase trypsin inhibitors (ATIs, which trigger innate immune activation), wheat germ agglutinin, and other proteins. A subset of people labeled NCGS are likely reacting to fructans or ATIs rather than gluten specifically. This doesn’t make their reaction less real, and it makes the label imprecise.
The Seronegative Celiac Question
Here’s the part of NCGS research that should genuinely concern anyone in this category: a meaningful proportion of people currently labeled with NCGS may actually have seronegative celiac disease.
Seronegative celiac is celiac without detectable antibodies on standard tests, sometimes due to IgA deficiency, sometimes for reasons not fully understood. It’s diagnosable on biopsy if the patient is eating gluten, and it carries the same long-term risks as classical celiac: nutrient deficiencies, osteoporosis, and increased risk of certain malignancies. Estimates from Volta’s group and others suggest that somewhere between 5% and 15% of people initially diagnosed with NCGS may, on closer investigation, have seronegative or atypical celiac.
This matters because the management overlap is incomplete. A person with celiac, even atypical, needs lifelong strict gluten-free eating, regular follow-up bloodwork, bone density screening, and screening of first-degree relatives. A person with NCGS may have more long-term flexibility and doesn’t necessarily need the same level of medical surveillance.
If you can tolerate a gluten challenge: If you haven’t been formally evaluated and you’re physically and psychologically able to undertake the gluten challenge, do consider it, ideally under specialist gastroenterology supervision. Knowing whether you’re celiac, seronegative celiac, or NCGS changes long-term medical care. The new Australian gluten-challenge-free blood test (currently in clinical trials) will eventually make this easier for those of us who can’t reintroduce gluten.
So What Do You Do With Non-Celiac Gluten Sensitivity, In Practice?
Whether you’re formally diagnosed with NCGS, self-diagnosed via elimination, untested, or seronegative, the practical management looks remarkably similar. The cleanest, most evidence-aligned approach is the one most people in this position eventually arrive at on their own:
1. Treat yourself with the seriousness celiac demands
Until you have certainty about which category you fall into, the safest default is to behave as though you might have celiac. That means strict gluten-free eating: not “mostly,” not “on weekdays,” not “unless I’m at a wedding.” The downside of being too strict is small. The downside of being too relaxed, if it turns out you’re actually celiac or seronegative celiac, is years of slow gut damage.
2. Build the diet on whole foods, not packaged “free-from” products
This is where most newly gluten-free people, with or without diagnosis, go wrong. Supermarket gluten-free products are often ultra-processed, low in fibre, and rely heavily on refined starches that don’t actually nourish a gut already trying to recover from inflammation. In this Complete Gluten-Free Diet Guide will find all you need to navigate in this free-from world.
There’s also a less-discussed concern with packaged gluten-free baked goods: many use bacterial transglutaminase, an enzyme that binds proteins. There’s literature review interest about the Association Between a Common Food Additive and Celiac Disease – transglutaminase enzymes may be relevant to gluten-related disorders, given that tissue transglutaminase is the autoantigen in celiac disease itself. The science is still developing, but a sensible precautionary stance, especially for anyone in the celiac/NCGS spectrum, is to minimise reliance on heavily processed gluten-free convenience foods and centre your diet on naturally gluten-free whole foods instead.
Whole-food, Mediterranean-style eating fits perfectly: vegetables, fruits, lean proteins, legumes, naturally gluten-free grains (rice, quinoa, buckwheat, millet, certified gluten-free oats), nuts, seeds, fermented foods, and good fats. None of these come in a packet labelled “free-from” because they don’t need to be.
3. Pay attention to what else might be going on
If you’ve gone strictly gluten-free and you’re still symptomatic, the issue may not be gluten alone. FODMAPs, histamine, nightshades, cross-reactive proteins (especially casein), and salicylates are all worth investigating. This is its own conversation, and one I’ll cover in the companion article, which is coming soon.
4. Re-test if circumstances allow
If new diagnostic tools emerge, particularly the gluten-challenge-free test currently being developed in Australia, reconsider getting tested. The clinical clarity of knowing whether you’re celiac or NCGS is genuinely useful for long-term health decisions, even if the day-to-day eating doesn’t change much.
5. Take your symptoms seriously, regardless of label
This is the philosophical heart of the article. You don’t need anyone’s permission to take your symptoms seriously. A negative blood test doesn’t override a body that consistently feels worse on gluten and better off it. Your evidence is your own response, repeated over months and years. That’s data.
On The Celiac vs Gluten Sensitivity Gatekeeping
There’s a particular flavor of online gatekeeping in gluten-free spaces that needs naming. Some celiac communities position non-celiac gluten sensitivity as a fashion, a hypochondria, a way of “diluting” what real celiacs deal with. The argument is usually that non-celiac gluten sensitivity readers don’t take cross-contamination as seriously, which makes restaurant culture more dangerous for celiacs.
There’s a kernel of legitimate concern there. Cross-contamination is genuinely dangerous for celiacs, and a culture that treats gluten-free as flexible can make eating out harder. But the response shouldn’t be to exclude the NCGS community; it should be to educate everyone, including NCGS readers, on why strictness matters.
The science doesn’t support a clean hierarchy where celiac is “real” and NCGS is “questionable.” Fasano and other senior researchers have been explicit that NCGS is a recognized clinical entity. The boundaries between celiac, seronegative celiac, NCGS, FODMAP-driven IBS, and ATI-driven innate immune reactivity are blurrier than the labels suggest. Many people move between categories as research evolves and as their own bodies change.
The inclusive position is the scientifically honest one: anyone whose body reacts negatively to gluten-containing foods deserves to be taken seriously, deserves access to good information, and deserves not to be patronised by either the medical establishment or the celiac community. Nobody deserves to suffer!
Gluten Sensitivity Navigation Map
1. If you suspect you react to gluten and haven’t been formally evaluated: see your GP and request celiac testing BEFORE removing gluten from your diet. Once you’re gluten-free, antibodies disappear, and biopsy normalises, making accurate testing much harder.
2. If your tests came back negative but you’re sure you react: ask about a structured elimination and reintroduction protocol with a gastroenterologist or registered dietitian, ideally following the Salerno criteria framework.
3. If you’ve been gluten-free for years already and a gluten challenge isn’t an option: behave as though you might have celiac, eat strictly gluten-free, build the diet around whole foods, and watch for new diagnostic options as the science advances.
4. Whatever your diagnostic situation: read the companion article on whole-food gluten-free eating, and the one on FODMAPs and other reactive food categories if your symptoms aren’t fully resolving.
Non-Celiac Gluten Sensitivity – Where To Go From Here
• The Complete Gluten-Free Diet Guide
• Newly Diagnosed Celiac — Now What? Your First 30 Days (the companion piece for those formally diagnosed)
• Hidden Gluten: Where It Hides and How to Spot It
• Whole-Food Gluten-Free Recipes
• When It’s Not Just Gluten: FODMAPs, Histamine, Nightshades and Other Reactive Foods (coming soon)
And if you’d like a free starter pack — my eBook with simple, whole-food gluten-free recipes designed to anchor a sustainable diet without packaged shortcuts — sign up to the newsletter below.
Fancy a Freebie?
Subscribe to my newsletter
and get your FREE eBook with 7 delicious gluten-free desserts!
*We will only send you gluten-free, lactose-free, refined sugar-free emails; you can unsubscribe anytime. Read our Privacy & Cookie Policy.



About the Author: Dani
Gluten-Free Recipes | Gut Health | Metabolic Health
Hi! I’m Dani, a Human Nutrition graduate with a strong interest in lifestyle medicine, gut health, metabolic health, UPF-free, whole-food, and gluten-free cooking. Your visit means the world to me!
I share simple recipes, nutrition tips, lifestyle experiences, and insights into living with food intolerances.
My story
My philosophy
This article isn’t medical advice. If you suspect you have a gluten-related disorder, see your GP and request appropriate testing before removing gluten from your diet. For ongoing care, work with a gastroenterologist, and ideally a registered dietitian/nutritionist experienced in gluten-related disorders.





